The SHA Scotland blog can now be found at http://www.shascotland.org/blog.
This blog site has all our posts prior to September 2014.
The SHA Scotland blog can now be found at http://www.shascotland.org/blog.
This blog site has all our posts prior to September 2014.
The impact of independence on NHS Scotland has caused some of the most impassioned debate in the whole campaign - despite it being a devolved issue. Objective analysis is hard to come by, but at least we now have some numbers, helpfully crunched by the respected Institute for Fiscal Studies.
Nicola Sturgeon has said that a 'Yes' to independence would free the Scottish NHS from an agenda of privatisation and public spending cuts. The 'No' campaign focuses on what iScotland’s finances would mean for NHS funding. Gordon Brown has said he wants to 'Nail the NHS lie' of the 'Yes' campaign.
The historical point IFS makes is that Scotland has not given the same priority the health spending as the UK, as this table illustrates.

For the future they point to the likelihood of downward Barnett consequentials of UK spending cuts that will make it harder to protect NHS spending. Unless, the Scottish Government is willing to use their existing and new taxation powers - something they appear reluctant to do.
Independence would give greater freedom to spend more, depending on the constraints of a currency union, should one be agreed. The capacity to do this depends on a range of assumptions over oil prices etc that are difficult to quantify. IFS has already set out their view on this, although it is challenged by Yes supporters, such as the Cuthbert's.
IFS conclude that, "in the short term, then, it is hard to see how independence could allow Scotland to spend more on the NHS than would be possible within a Union where it will have significant tax raising powers and considerable say over spending priorities."
They also say the longer-term outlook is more difficult for them to quantify, "a combination of the eventual fall in oil revenues and an ageing population could make for a tougher fiscal outlook for Scotland than the rest of the UK and hence less room for additional spending on things like the NHS." They concede this could be offset by faster economic growth in iScotland, but that is not certain, by any means.
There are some mixed messages in the latest batch of NHS Scotland statistics. Workforce numbers are up last year, although still less than before the crash and vacancies are high. Some health boards are struggling to meet waiting time targets and most missed the four hour A&E wait target. Perhaps most challenging is increased bed blocking.
The workforce statistics show that the total number of NHS Scotland staff in post increased last year with 135,881 whole time equivalent (WTE) and 159,058 headcount on 3 June 2014. The annual increase in staff of 1.9% WTE is mainly due to increases in nursing and midwifery (1,309.6 WTE), administrative services (345.5 WTE), medical (286.2 WTE) and allied health professions (226.4 WTE).
Welcome though this year’s increase is, it’s worth remembering that the highpoint for NHS staff in Scotland was September 2010 when the WTE was 135,964. When the council staff transferred into NHS Highland are taken into account, the NHS is still around 1000 staff down since the financial crash.
In addition, the total number of vacancies remains high. Consultants 346.7 WTE, a rate of 6.9%; Nursing and midwifery 1,865.3 WTE, a rate of 3.1%; Allied health professions 481.2 WTE, a rate of 4.1%. The Health Secretary argues that this is a mixture of hard to fill specialists and increasing staff numbers. Others suspect that some health boards are balancing their books by deliberately not filling vacancies.
The statistics on waiting times and bed blocking highlight significant regional variations. Grampian, Lothian and Forth Valley missed a target to treat the majority of people within 18 weeks. Only two health boards managed to treat most patients in A&E departments within four hours. Five health boards missed an interim target to treat 19 out of 20 patients within that time frame. Only five of the 14 health boards have achieved the 26 week waiting time for treating children and young people who need care for mental health problems.
175 patients remained in hospital six weeks after being fit enough to be discharged. The main reason given was the lack of a place in a care home. The target is that no patient should be delayed in hospital for more than four weeks and that will fall to two weeks by April next year. 518 patients are waiting more than two weeks at present. In total, nearly 900 patients are in hospital when they have been assessed as ready for discharge - the equivalent of Scotland’s largest hospital.
All these numbers have increased over the last year and exclude the 300+ patients classified as Code 9, which means there is an approved cause for their delayed discharge. Interestingly, there are significant regional differences as the chart below highlights. This will be a key challenge for the new integration boards.

Some sad news that our Vice-Chair Ali Syed has passed away after a long illness. Ali was a stalwart of SHA Scotland for many years, serving as Chair and then in retirement as Vice-Chair. He also served on the SHA UK Central Council.

He had an outstanding NHS career in cancer care, latterly at the Beatson Centre in Glasgow.
Ali was a trade union activist for many years holding a range of posts in UNISON health branches and in Glasgow Trades Council. His trade union values shone through in all his work, including the many causes he took up - not least the plight of the Palestinian people.
He was Labour to the core and made many contributions at Scottish Labour Party conferences - even when he wasn't even a delegate. Nothing stopped Ali when he had something to say!
He will be sadly missed by all his comrades and the very many people he helped. Our thoughts are with his family.
He will be interred at Glasgow Central Mosque at 1:30pm on Tuesday 26th August.
It is perhaps surprising that a devolved issue, the NHS, has become the latest 'battleground' issue in the referendum campaign. The Yes campaign, desperate to move away from the currency issue, are issuing press releases almost daily on the issue. Apparently, only a yes vote will save the NHS.
There appears to be two grounds on which this claim is based.
Firstly, that the English NHS is being privatised and therefore this will be forced on Scots, who have rejected the marketisation of health services. The primary difficulty with this argument is that the NHS is a devolved service, so it's the Scottish Parliament that decides the structure of the NHS. And that's exactly what they have done. Dave Watson's blog on this site reminds us how that happened, not by an SNP administration for whom falling out with Westminster is compulsory, but by Scottish Labour ministers who went in a different direction to that of their UK counterparts.
The minister who we have most to thank for that is Malcolm Chisholm. The MSP respected even by his political opponents and the least likely to follow the party line on anything. His view of the Yes campaign argument is: "This has to be not just the biggest lie of the Referendum campaign but the biggest political lie of all my years in politics."
Somewhat ironically, if there is a threat to the NHS as a public service it comes from the EU and the proposed TTIP treaty with the USA. But of course the Yes campaign will not have us exiting the EU. It would also possibly be churlish to point out that spending on private health care by NHS Scotland has increased by 37% since the SNP came to power.
The second argument is that a privatised English NHS will result in a cut in spending and therefore a consequential cut in Scotland's NHS through the Barnett formula. There are frankly more holes in this argument than a Swiss cheese.
Anyone who has studied market driven health systems knows that transaction costs increase. More money is spent, not on care, but on administration. The SNP trumpet the £1bn efficiency savings target for the English NHS, that they claim means £100m taken from the Scottish budget. They forget to mention that NHS Scotland also has efficiency savings targets, but as in England they get ploughed back into the NHS. The net result is no budget cut and therefore no Barnett consequentials. Even if there was, the consequentials would be for the Scottish budget as a whole, not the NHS in Scotland.
In fact, the opposite has been the case. Because the Tories have largely protected health spending in England, Scotland's budget has not been cut as much as UK budget as a whole. Small comfort, but it does demonstrate that even the Tories recognise that cutting health spending is electoral suicide for them in England. As the Scottish Government explanation for the Scottish health budget increase says, "This is the full amount of the budget consequentials arising from the increase to health in England and delivers on the Scottish Government’s commitment to pass on the resource budget consequentials in full to the health budget in Scotland."
For an objective view on these points you can read the ITV or the BBC analysis, amongst many others. Even Yes leaning academics have pointed to the huge flaws in the argument.
If there is an argument here, it is that the Tories do want to roll back the state with their austerity programme. But that is a political choice that voters across the UK can reject. There is also the small matter of how Scotland's finances might look after independence. A valid debating point, but not specifically about the NHS.
There are many valid arguments for independence and SHA Scotland has covered these in its latest journal. However, the NHS arguments are hugely cynical, the Yes campaign's version of 'Project Fear'. Cynical because most people don't understand how our services are structured and financed, but they do value our NHS. The referendum debate deserves better from those who understand these matters all too well.
Happy 66th Birthday to the NHS in Scotland! While the NHS is great at treating illness, the greatest health challenge in Scotland is health inequality. That requires coordinated action across our public services.
To commemorate this birthday, UNISON Scotland has published a paper on health inequalities in Scotland. I drafted this paper as our submission to the Health Inequalities Review commissioned by Neil Findlay MSP. The review starts from the premise that Scotland’s health inequalities are the unjust differences in life expectancy and these differences are determined by socio-economic position, caused by the unfair distribution of income, wealth and power. Tackling this inequality is arguably the greatest challenge we face as a society.
Overall life expectancy has increased in Scotland in recent years, but continues to be closely associated with deprivation. The average life expectancy of men living in the least deprived areas remains around 11 years higher than in the most deprived areas. There have been many reports describing this problem, but less focus on solutions. That's why this paper focuses on policy recommendations that we believe could make a real difference.
We start with the structural changes that are needed to break down silo working. We need to assess every policy against national indicators on health inequality, but it is at local level, working through Community Planning Partnerships where joined up working needs to become a reality. As Christie recommended, staff and service users should be fully engaged in delivering positive health outcomes.
While health inequality requires cross service action, that doesn't mean we should ignore health actions. The paper sets out a range of actions that address public health concerns around smoking, drugs and alcohol. Social care in Scotland is a national disgrace and much more needs to be done on improving mental health. We also need to ensure that NHS resources are targeted on areas of greatest deprivation. The NHS must be at its best where it is needed the most.
Finally, we set out a range of broader actions. These include action in the workplace through occupational health, health and safety, and measures to tackle worklessness. Improving our environment through design, better housing, sustainable transport policies, as well as measures to tackle climate change. Preventative spending should be at the core of our approach with quality early years provision, followed throughout the education journey to further and higher education.
Eradicating fuel poverty is vital to health inequality. That means raising incomes, freezing energy prices and effective energy efficiency measures. UK child poverty rates are predicted to rise to 24% by 2020, resulting in an additional 50,000 children in Scotland living in poverty. So welfare reform and increasing wages are an essential element of this strategy.
A comprehensive strategy starts with a recognition that health inequalities are caused by socioeconomic inequality. Building on that analysis, we must take action to narrow wealth and income inequality, not just increasing income at the bottom. Other actions require a new structural approach that places health inequalities at the centre of public policy, leading to a range of practical measures that can alleviate and then eradicate health inequalities.
Dave Watson
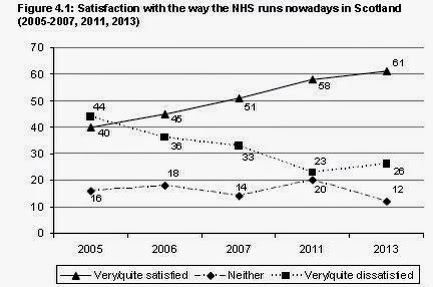
Public satisfaction with Scotland's NHS continues to rise, while support for privatisation falls.
New findings from the Scottish Social Attitudes Survey (SSAS) 2013 have found satisfaction with Scotland’s NHS increased by over 20 per cent since 2005. The official survey of around 1500 Scots found that 61 per cent of people in Scotland were either very or quite satisfied with the NHS, compared with only 40 per cent in 2005. This high level of satisfaction is reflected in the patient experience as well. In last year’s Health and Care Experience Survey, 85 per cent of Scottish inpatients say their overall care and treatment was good or excellent, and 87 per cent also rated the overall care from their GP surgery as good or excellent too.
The survey authors also speculate that the reduction in NHS satisfaction levels in the UK since 2011 may be due in part to concerns about the organisational reforms in the English NHS following the introduction of the Health and Social Care Act in 2012
Scots also continue to reject the marketisation of care. In this survey, the majority of people (59 per cent) also thought the government would provide better quality care services than the private sector. There has even been a drop in support for charities running care services. It was always low for hospitals and very low for the private sector. Private sector involvement in the NHS may be minimal in Scotland, but it is common in the social care sector, particularly residential and home care.
This survey shows that opposition to the marketisation of health and care remains strong in Scotland and that most Scots believe that cooperation is the best way to run our NHS.
Given the downward spiral of the NHS in England, we should give full credit to the Scottish Labour administrations who ensured that Scotland exited the road to health marketisation.
A few recent events made me think about the recent history of the NHS in Scotland. Firstly, the announcement that Malcolm Chisholm MSP is to retire at the next election. He was the Labour health minister who abolished NHS trusts in Scotland.
Secondly, an answer Nicola Sturgeon MSP gave at a recent UNISON referendum hustings comparing the NHS in Scotland and England. She didn't quite say that this was entirely down to the SNP, but those not aware of the history might have interpreted it that way. That's not to say that she wasn't a very good health minister herself and strongly opposed to marketisation. However, she was continuing the work of others. It also reflects the fact that there is not an ideological divide between Scottish Labour and the SNP on health.
Thirdly, a trip to our UK health conference reminded me just how bad NHS England is!
Following the 1997 general election Labour came into government and quickly initiated the devolution referendum that resulted in the first devolved administration in 1999. In April 1999 they set the path to reform by halving the number of NHS trusts in Scotland from 47 to 28. Susan Deacon was the first health minister and everyone was left in no doubt that the market was not the future for health care in Scotland. I spent some eighteen months on secondment to the health department during this period and then served on her advisory board. I'll be circumspect, as I am probably still covered by the Official Secrets Act and the key players are still alive, but let's just say there was some institutional resistance to the direction of travel!
None the less important steps were taken to build cooperation in the NHS rather than competition. Market testing was dropped and services started to come back in house. This included a new HR strategy (the primary reason for my secondment) that introduced partnership working into the NHS. A model that survives to this day and has been rated as probably the best of its type in the world.
At the end of 2001, Malcolm Chisholm took over as health minister and he took over the reform process that resulted in the NHS Reform Act of 2004. This Act formally abolished trusts and established a duty of cooperation. We had Community Health Partnerships for primary care and staff governance was given a statutory footing.
It is often said that Scottish Labour is dictated to by 'London Labour' - largely a myth in my extensive experience of the policy making process. However, it is certainly the case that when New Labour in England reintroduced elements of NHS marketisation there was pressure to follow the same model in Scotland. What is less well known is that Scottish Labour ministers resisted that pressure. I remember one Blairite special advisor in the run up to the UK general election complaining, that the Tories said if their reforms were so good why didn't the Scots adopt them - could we not just sound a bit like them? He was firmly told that the answer was, 'it's devolution stupid!'. However, part of the problem was that ministers were told not to highlight differences and as a consequence they have never got the credit they deserve.
The last Labour health minister, Andy Kerr, went against Gordon Brown's decision to defer a PRB award (topical again this month) and bought, what is now the Golden Jubilee Hospital, into public ownership. Even if he didn't appreciate our press release welcoming the hospital's 'nationalisation'!
The one issue that didn't get resolved was stopping the big PFI hospital projects that had been started and some smaller ones that joined the programme. Ministers like Malcolm Chisholm didn't like PFI, but they were told it was 'the only game in town', due to off balance sheet funding. Wrong in principle and practice and sadly a lesson not learnt to this day, as the present Scottish Government has one of the biggest PFI programmes in Europe.
The first two post devolution administrations didn't get everything right and certainly not over PFI. However, they made crucial decisions over a partnership approach to health through cooperation rather than competition. Health ministers like Susan Deacon, Malcolm Chisholm and Andy Kerr, supported by the wider cabinet, made these decisions and kept to this approach despite political pressure from elsewhere. When we see what's happening to the NHS in England, we should remember to say, thanks very much comrades!
Dave Watson
Health and care integration is right in principle but it will take more than moving the managerial deck chairs around to deliver quality care.
I took a day away from the STUC in Dundee to make a day trip to Brighton to speak in panel discussion on health and care integration at the UNISON UK health conference. I was giving the Scottish perspective on what is a similar challenge across the UK.
The context for integration is pretty similar across the UK. Demographic change is even more acute in Scotland with 25% of the population over 65 by 2035 and an 80% increase in the over 80s. Today's FT had an interesting UK Statistic reporting that centenarians will grow from 14,000 in 2013 to 111,000 in 2037. It will at least keep the Queen busy. Their overall message was let's embrace longevity, it's a good thing. That said, we can't ignore the financial pressures that have resulted, in social care at least, in a race to the bottom as UNISON Scotland's Time to Care report highlights.
There have been efforts to promote care integration since the 'joint finance' initiative in the 1970s, with admittedly limited success. An Audit Scotland report found few examples of effective joint planning. The long waits for patient discharge have largely gone, but 837 patients are still in Scottish hospitals who should not be. That's the equivalent of the Southern General Hospital. The Scottish public service model, based on collaboration not marketisation, should enable joint working, but as the Christie Commission found this hasn't always been achieved.
The new integration model is outlined in the Public Bodies (Joint Working) Act, to be implemented in April next year. This permits two broad models. Lead agency and body corporate bring in councils and health boards together in Health & Social Care Partnerships. Everywhere other than Highland are likely to go for the body corporate model. They will be run by an Integration Joint Board with at least 3 council and 3 Health board members plus non-voting members from the voluntary sector, trade unions and patient groups. Each Board has to develop integration plan (services, budgets) and a three year Strategic Plan. There will also be Locality Planning Groups below council level. All of these plans have to approved by minister who has extensive powers and will set national outcomes and lead an accountability process. No staff will transfer to the new bodies, they will remain employed by councils and health boards.
UNISON Scotland welcomes the less prescriptive model than first envisaged, but remains concerned about the extensive ministerial powers that could be another force for centralisation. International studies show that local implementation is the key to successful integration. The staffing provisions are minimal, but after our Bill lobby a partnership group has been established to address workforce issues.
Outsourcing remains a concern as home care is the most outsourced public service Scotland and we don't want to see that extended any further - certainly not into NHS provision. The financial provisions in the Act are weak with little indication of how growing care needs are to be funded. The savings identified in the Christie report on unplanned admissions have already been absorbed into rising, not reducing NHS bed requirements. I would also argue that GPs are weakly integrated into new system and they can be a big driver for admissions to hospital.
Finally, for the future more work is needed on the detailed secondary legislation and local plans. UNISON's short term focus is on effective joint branch working and developing skills. The industrial relations cultures in health and local government are also very different.
In the longer term, I argued that we need to address three key care issues. Improve the social care workforce as set out in UNISON's Ethical Care Charter. Find a way of funding care at the level we are going to need. And develop a new social contract that sets out the responsibilities of the state and the citizen. Vague concepts like co-production and asset based approaches need more definition.
Dave Watson




